Understanding Cellulogia as a Structural Skin Condition
Cellulogia refers to a structural alteration of subcutaneous tissue that affects skin topography. Medical literature often associates cellulogia with gynoid lipodystrophy, yet the term emphasizes tissue architecture rather than cosmetic appearance. The condition involves adipocytes, fibrous septa, microcirculation, and extracellular matrix interaction. Authoritative dermatology sources such as the American Academy of Dermatology and the National Institutes of Health describe this condition as benign and non-inflammatory. Cellulogia affects skin texture without causing systemic disease, pain syndromes, or infectious processes.
Cellulogia primarily appears in regions with hormonally influenced fat distribution. Thighs, gluteal areas, hips, and lower abdomen demonstrate the highest prevalence. The condition develops independently of body mass index. Lean individuals also present with structural changes consistent with cellulogia.
Defining Cellulogia Using Medical Parameters
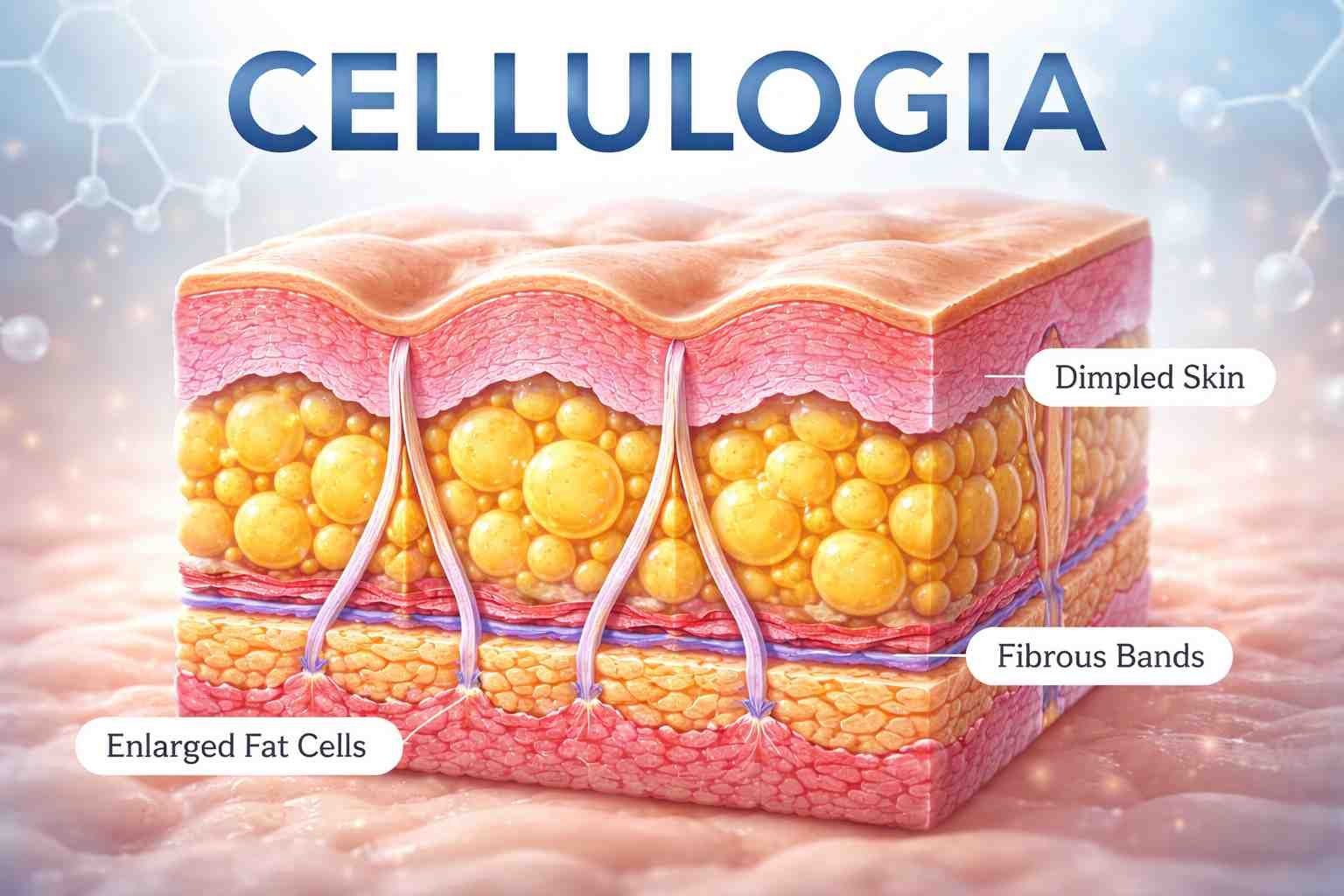
Cellulogia is defined by connective tissue tension and adipose protrusion. Adipocytes expand vertically against the dermis. Fibrous septa restrict lateral expansion. This interaction produces visible surface irregularities. Histological examination confirms septal thickening, reduced collagen elasticity, and altered capillary density. The Mayo Clinic differentiates cellulogia from inflammatory skin disorders due to absence of erythema, heat, or leukocytic infiltration.
Cellulogia represents a tissue configuration rather than a disease state. This distinction is critical for diagnostic accuracy and treatment expectations.
Biological Mechanisms Behind Cellulogia
Adipose Tissue Behavior
Adipocytes store triglycerides under endocrine regulation. Estrogen modulates lipid accumulation in gynoid regions. Enlarged adipocytes increase interstitial pressure. Pressure pushes against dermal layers. This mechanical effect contributes to uneven skin relief.
Connective Tissue Architecture
Fibrous septa anchor skin to deeper structures. In females, septa align perpendicularly to the skin surface. This orientation facilitates upward fat displacement. Reduced collagen flexibility amplifies the visible effect. Research published in the Journal of Investigative Dermatology confirms gender-specific septal patterns.
Microcirculation and Lymphatic Flow
Capillary compression reduces oxygen delivery. Reduced oxygen favors fibrotic remodeling. Lymphatic drainage inefficiency increases extracellular matrix density. Increased density decreases tissue compliance. These factors combine to stabilize the irregular surface pattern.
Hormonal Influence on Cellulogia Development
Hormonal signaling directly influences cellulogia expression. Estrogen receptors concentrate in thigh and gluteal adipose tissue. Estrogen increases lipogenesis and decreases lipolysis locally. Insulin supports adipocyte nutrient uptake. Catecholamines regulate fat mobilization but demonstrate reduced receptor sensitivity in affected areas.
Life stages such as puberty, pregnancy, and menopause correlate with structural shifts. The Endocrine Society recognizes hormonal modulation as a primary determinant of regional fat behavior rather than total fat mass.
Genetic and Anatomical Contributors
Genetic factors regulate collagen synthesis, dermal thickness, and adipocyte distribution. Genome-wide association studies referenced by the NIH associate connective tissue gene variants with increased susceptibility. Skin thickness, elastic fiber density, and fat compartment size demonstrate heritable patterns.
Anatomical fat distribution follows a gynoid pattern in most females. Pelvic and femoral regions prioritize triglyceride storage. This anatomical preference increases adipocyte density and septal strain.
Clinical Classification of Cellulogia
Dermatology uses standardized grading systems to describe severity. The Nürnberger–Müller scale remains the most cited.
| Grade | Clinical Presentation |
|---|---|
| Grade 0 | Smooth skin at rest and compression |
| Grade 1 | Smooth skin at rest, dimpling on compression |
| Grade 2 | Visible dimpling at rest |
| Grade 3 | Deep nodules, pronounced surface irregularity |
See More: Prostavive Colibrim: Advanced Insight Into a Modern Prostate Support Formula
Diagnostic Approach to Cellulogia
Diagnosis relies on physical examination. Visual inspection identifies surface changes. Palpation assesses nodularity and tissue tension. Photographic documentation supports longitudinal comparison. Imaging modalities such as ultrasound or MRI confirm septal thickness and adipose protrusion but remain non-essential for routine evaluation.
Laboratory testing does not contribute to diagnosis. The absence of systemic markers differentiates cellulogia from metabolic or inflammatory conditions.
Distinguishing Cellulogia From Similar Conditions
Accurate differentiation prevents misclassification.
| Condition | Key Differentiator |
|---|---|
| Cellulitis | Infection, erythema, systemic symptoms |
| Lipedema | Symmetric painful fat accumulation |
| Lymphedema | Persistent swelling and pitting |
| Panniculitis | Inflammatory nodules |
Evidence-Based Management Strategies
Topical Interventions
Topical formulations target superficial structures. Caffeine promotes localized lipolysis. Retinoids stimulate collagen synthesis. Clinical reviews by the AAD report mild surface smoothing with continuous use. Effects remain temporary due to lack of deep tissue remodeling.
Mechanical and Manual Therapies
Manual lymphatic drainage increases transient fluid movement. Vacuum-assisted massage alters septal orientation temporarily. Shockwave therapy stimulates fibroblast activity. The European Academy of Dermatology and Venereology documents short-term textural improvement.
Energy-Based Technologies
Radiofrequency induces collagen contraction through thermal energy. Laser-assisted devices disrupt fibrous septa. Focused ultrasound modifies adipocyte structure. NIH-funded trials demonstrate measurable reduction in dimple depth following controlled treatment protocols.
Injectable Modalities
Collagenase clostridium histolyticum enzymatically cleaves fibrous septa. The FDA approves this treatment for specific grades. Randomized clinical trials show statistically significant surface smoothing with predictable outcomes.
Role of Physical Conditioning
Resistance training increases underlying muscle volume. Increased volume provides mechanical support to overlying tissue. The World Health Organization associates physical activity with improved tissue composition. Exercise modifies visual prominence without altering septal architecture.
Nutritional Considerations in Research
Protein intake supports collagen turnover. Micronutrients contribute to connective tissue metabolism. The NIH Office of Dietary Supplements confirms no dietary intervention reverses cellulogia. Nutrition supports tissue health without structural normalization.
Prognosis and Long-Term Outlook
Cellulogia persists across adulthood. Severity fluctuates with hormonal status and connective tissue changes. The Mayo Clinic classifies the condition as chronic yet stable. No systemic complications arise from the condition.
Emerging Research Directions
Current research investigates extracellular matrix remodeling and microvascular regulation. Clinical trials explore biologic agents and hybrid energy devices. The NIH Clinical Trials Registry documents ongoing studies targeting septal elasticity and adipocyte signaling pathways.
See More: Understanding Doctiplus as a Digital Healthcare Infrastructure
Frequently Asked Questions About Cellulogia
What exactly is cellulogia?
Cellulogia is a structural alteration of subcutaneous tissue involving adipocytes, connective septa, and microcirculation.
Is cellulogia a medical disease?
Cellulogia is classified as a benign structural condition, not a disease or infection.
Can thin individuals have cellulogia?
Cellulogia appears independently of body weight and affects individuals across body compositions.
Are treatments permanent?
Current treatments provide variable cosmetic improvement without permanent tissue normalization.
Does cellulogia indicate poor health?
Medical authorities confirm cellulogia has no association with systemic illness.
Conclusion
Cellulogia represents a structurally defined alteration of subcutaneous tissue involving adipocytes, fibrous septa, microcirculation, and extracellular matrix organization. Medical and dermatological authorities consistently classify cellulogia as a benign, non-inflammatory condition that affects skin surface morphology without systemic health consequences. The condition develops independently of body weight and reflects anatomical, hormonal, and genetic determinants rather than lifestyle failure.
Clinical evaluation confirms that cellulogia arises from the interaction between adipose tissue expansion and connective tissue rigidity. Hormonal signaling, particularly estrogen modulation, explains its regional distribution and high prevalence. Diagnostic clarity depends on visual and tactile assessment, supported by established grading systems that describe severity without implying disease progression.
Current management strategies focus on measurable structural modification and temporary surface improvement. Topical agents, mechanical therapies, energy-based devices, and injectable modalities demonstrate variable efficacy based on tissue architecture and treatment protocol. No intervention achieves permanent normalization of tissue configuration, reinforcing the importance of accurate expectations grounded in medical evidence.